



Point-of-care testing (POCT) goes a long way toward helping institutions improve patient care by returning fast and reliable results near patients, thereby enabling prompt clinical interventions.
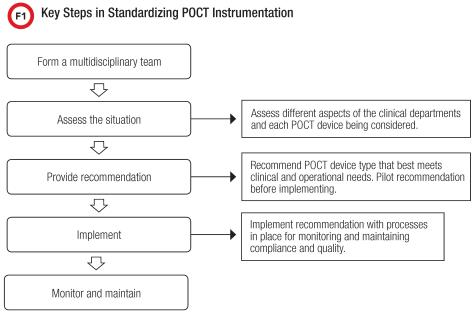
POCT’s vital role in patient management makes it popular across clinical settings but often with different device types for the same test. Our institution is no exception to this POCT device creep, as at one point we had more than four types of blood gas analyzers, three table tops and one hand-held. Realizing that this confounded many of our quality and efficiency aims, we undertook a deliberate and durable process to standardize these instruments, using the general process outlined in Figure 1.
Our first step was to acknowledge the challenges having multiple device types presented. The devices’ different processes and steps put us at risk for decreased compliance with accreditation standards, if for example, required quality control (QC) was not run. This also increased the risk for pre-analytical error, as all the instruments weren’t interfaced owing to the expense involved. At the same time, having multiple types of blood gas analyzers actually increased our costs. A smaller volume of tests purchased from four vendors combined with yearly maintenance fees meant that our overall costs were higher than they would have been if we just had one instrument type.
Finally, using non-interfaced analyzers put a lot on our respiratory therapists (RTs) who were the operators for the inpatient floors. Our inefficient, non-interfaced devices and processes disrupted their workflows and required many manual steps. So our journey to a single type of POCT blood gas analyzer promised us improved efficiencies and quality as well as cost savings.
In the Beginning, Data
Our POCT team started our efforts with data. We clearly outlined the issues involved, compiled non-compliance and error data, existing cost and potential savings information from manufacturers, and determined our test volume. We looped in our hospital compliance officer about the risks associated with the status quo, then talked individually to stakeholders in each area that had blood gas analyzers. Our goal was to get them to see the serious issues we faced as well as the advantages of moving to one instrument type.
Having gained the support of these individuals, we established a multidisciplinary team tasked with identifying a blood gas analyzer that would meet the needs of all areas. This team consisted of providers, administrative directors, managers, and POCT operators from the different areas, including RTs.
The team rolled up its sleeves and did an extensive analysis, considering the pros and cons of each instrument and documenting the clinical needs of all users. Concurrently, the lab performed analytical comparisons of all four blood gas instruments, distilling and clearly communicating this information to the team and to stakeholders.
After reviewing clinical and operator needs, analytical performance, and division preferences, we determined no single instrument type would meet the needs of all areas. In the end, the team recommended one hand-held and one table-top analyzer.
Going with a single type of table-top analyzer would meet the clinical needs of all areas, including offering co-oximetry and measured hemoglobin, both unavailable via hand-held. However, this would run contra to the hospital’s goal of keeping care at patients’ bedsides and improving RTs’ workflow because we kept the table-top analyzers in a central location on patient floors and RTs had to walk to and from the analyzers for each test.
Adding the already interfaced hand-held analyzer would enable near-patient testing, decrease pre-analytical errors associated with delays in testing, and simplify RT workflow. Nurses also were trained to perform testing on the hand-held, giving additional relief to RTs.
Consolidating to a single table-top analyzer also afforded the hospital cost savings from decreased maintenance fees, more consumables purchased at lower prices thanks to increased test volume, and a more affordable cost of interfacing just a single type of analyzer.
A Piloted Approach
Armed with our recommendation, we moved forward with a 5-month pilot implementation in an area of the hospital with high provider and staff buy-in for the change. During the pilot we assessed several factors including: ease of instrument use; personnel satisfaction; number of instruments needed; RT workflow; compliance; error rate; test volumes; and lab test utilization.
At the pilot’s conclusion, the team reviewed the data we collected and discussed it with all stakeholders to determine whether it was appropriate to adopt both instruments hospital-wide. With a green light to proceed, we focused on educating providers on appropriate test utilization and planned an extensive program of personnel training, since many staff members had not used the instruments. To ensure that we had instrument availability, we submitted a budget for approval early-on for the approved new instruments and a data management system.
Next, we set a go-live date that all stakeholders had approved, and from there we have continued to monitor and maintain these two types of blood gas analyzers.
Though our process was long and painstaking, our efforts paid off and we achieved our aims. In my view, one of the most critical factors in our success was in identifying the stakeholders in each affected area early and gaining their support, which helped an already challenging situation go smoothly.
Author: Brenda Suh-Lailam, PhD, DABCC, FACB, is assistant director of clinical chemistry and mass spectrometry and director of point-of-care testing at Ann & Robert H. Lurie Children’s Hospital of Chicago, and an assistant professor of pathology at Northwestern University Feinberg School of Medicine.
Source: AACC





{kind=link}